
Hemorrhage, the rupturing of a blood vessel within the brain, is the second most common type of stroke, seriously affecting millions of people annually. Yet, despite its high burden on society and prevalence rate, hemorrhaging continues to be a condition which cannot be fully remedied by present medicine and pharmaceutical supplements alone, making it challenging for people who have survived a hemorrhagic episode to bounce back fully and return to their daily lives. Therefore, more research is needed, in order to enable scientists to understand the mechanisms of hemorrhaging, find ways to prevent it in high-risk patients, and establish more effective methods for treating patients which are in the post-hemorrhage stage and help them recover their cognitive functions as quickly as possible.
In this article, we will go over industry-standard rodent models commonly utilized by researchers for studying hemorrhages (while assessing the advantages and disadvantages) and explore the mazes which the animals go through during cognitive and behavioral testing.
But, first, let’s review a few things about hemorrhages.
Hemorrhage: A specific type of stroke
Stroke, a potentially fatal medical condition where the brain’s blood flow is suboptimal (due to vessels rupturing or being blocked, thus leading to cell death), has been deemed as the second leading cause of death in the world and is one of the top conditions which cause disability. The two categories of stroke are hemorrhage (refers to bleeding in the brain) and ischemic (refers to lack of blood flow). About 10% to 20% of all stroke cases are hemorrhages.[1]
A blood vessel within the brain can rupture, or hemorrhage, as a result of a pre-existing complication (such as a tumor, trauma, drug intake, or unsuccessful surgery). When something causes the rupture, it is classified as a secondary hemorrhage. However, when there is no clear-cut cause for the rupture, then this is labeled as a primary hemorrhage and it is considered to be the most frequent kind of hemorrhage.
Hemorrhaging can occur anywhere in the brain, including the brain matter (referred to as an intracerebral hemorrhage) and the membranes that cover and shield the brain (typically referred to as a subarachnoid hemorrhage).
When an artery or vessel bursts in the brain, the bleeding spreads to nearby tissues and kills the brain cells. Blood can also cause irritation which in turn leads to brain swelling, known as cerebral edema. When a lot of blood is concentrated and becomes mass-like, it is referred to as a hematoma. Brain tissue is further stressed due to the subsequent increase in pressure which then reduces natural, vital blood flow, thus putting brain cells in an even more critical condition.
The deadly impact on brain cells is later observed in serious alterations in behavior and cognitive decline.
Since hemorrhaging cannot be directly studied in humans due to ethical concerns, animal models are indispensable and incredibly crucial for advancing the field and developing therapeutic methods.
General Overview of Hemorrhage Animal Models
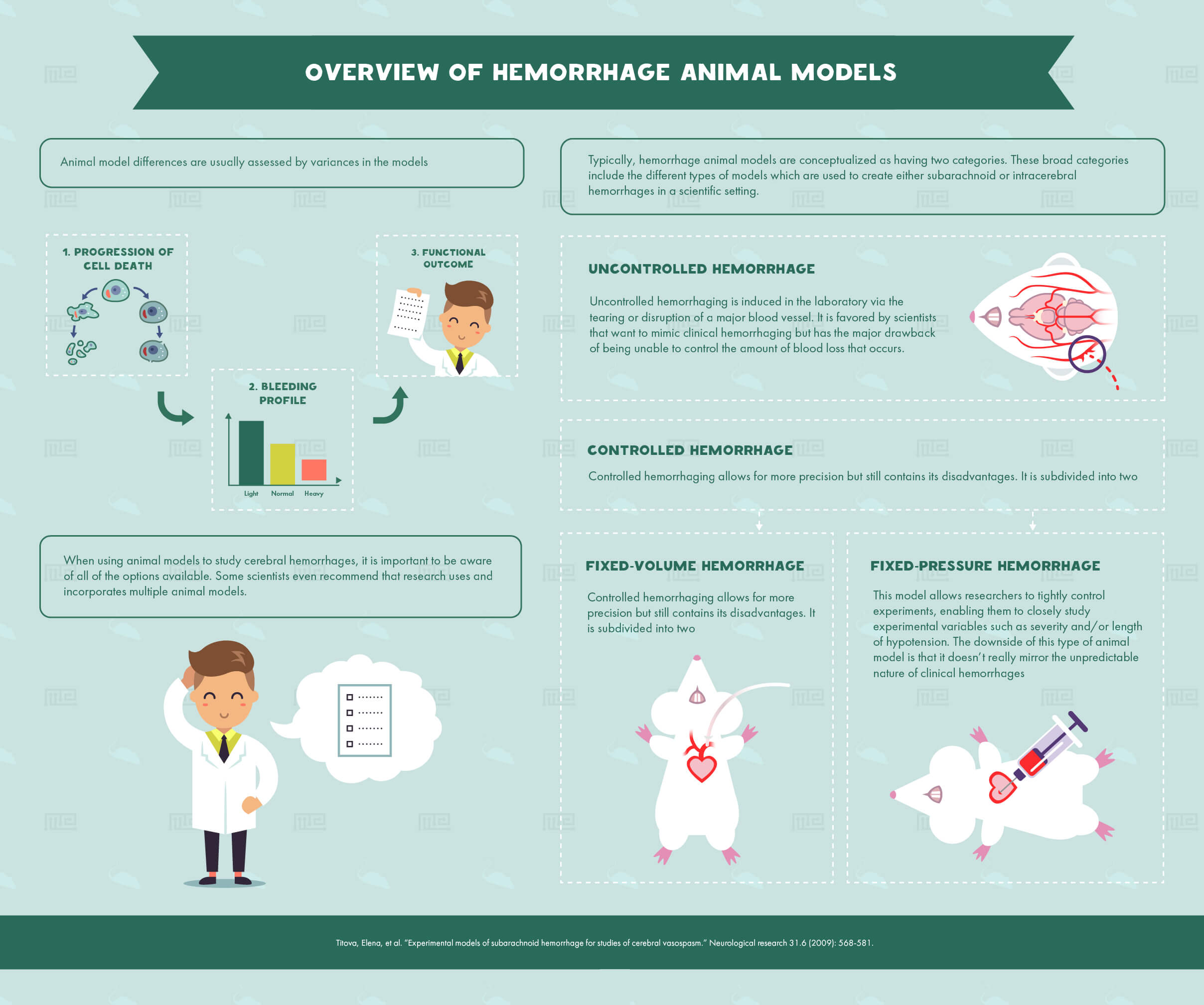
Animal model differences are usually assessed by variances in the models’
- Progression of cell death
- Bleeding profile
- Functional outcome
When using animal models to study cerebral hemorrhages, it is important to be aware of all of the options available, in order to select the most appropriate one. Some scientists even recommend that research uses and incorporates multiple animal models, in order to investigate potential treatment methods as fully as possible.
Typically, hemorrhage animal models are conceptualized as having two categories, classified as either uncontrolled or controlled. The latter category is subdivided to include fixed-volume and fixed-pressure hemorrhages, as summarized by the following outline:
- Uncontrolled hemorrhage
- Controlled hemorrhage
- Fixed-volume hemorrhage
- Fixed-pressure hemorrhage[2]
These broad categories include the different types of models which are used to create either subarachnoid or intracerebral hemorrhages in a scientific setting. The models will be discussed in greater detail soon.
Uncontrolled Hemorrhaging Animal Model
Uncontrolled hemorrhaging is induced in the laboratory via the tearing or disruption of a major blood vessel. Uncontrolled hemorrhaging is favored by scientists that want to mimic clinical hemorrhaging but has the major drawback of being unable to control the amount of blood loss that occurs.
Controlled Hemorrhaging Models: Fixed-Volume and Fixed-Pressure
Controlled hemorrhaging, on the other hand, allows for more precision, but still contains its disadvantages. In fixed-volume hemorrhages, about 25-45% of blood volume is lost through a cardiac puncture or an arterial catheter. By controlling blood volume, researchers can closely study any subsequent compensatory mechanisms, such as changes in blood gases, which occur within the organism. However, the negative aspect of this model is that there is a high amount of variability in the hemodynamic response; how nutrients and oxygen are delivered to cells and neurons, which occurs as a result of blood volume loss.
Fixed-pressure hemorrhage models, a different type of controlled hemorrhaging, keep blood pressure at 20-50 mmHg for 30 minutes to three hours (depending on the experiment) through the continuous withdrawal of blood. The fixed-pressure hemorrhage model allows researchers to tightly control experiments, enabling them to closely study experimental variables such as severity and/or length of hypotension. The downside of this type of animal model is that it doesn’t really mirror the unpredictable nature of clinical hemorrhages.[2]
Subarachnoid Hemorrhage Animal Models
Subarachnoid hemorrhaging occurs in the subarachnoid space on the brain. Subarachnoid hemorrhage (SAH) models are commonly used within the research field, each with their strengths and weaknesses.
SAH Models In Rats
Due to the advancement of imaging technology making this possible, including cerebral angiography, MRI, and digital subtraction angiography, rats have become a popular choice for studying SAH and cerebral vasospasms.
Rats, over the past few years, have become the most commonly used experimental animals for studying subarachnoid hemorrhaging, becoming more popular than felines and k-9’s. Below is an overview of a few popular hemorrhage models in rats.
The Transclival Puncture Model in Rats
The puncture model is a relatively early model in which the basilar artery is punctured via the midline portion of the clivus. Using this model, one can predict what the mortality rate and the severity of the vasospasm will be based on the device’s diameter which was used to create the perforation on the artery. Since the rat transclival puncture model was established, a few steady characteristics have emerged. For example, in the transclival puncture model, vasospasms are most evident at the 24- and 48-hour time frame after surgery and rats return to control levels after 72 hours. Furthermore, the vasospasm has been described as being biphasic and as a strong indicator of mortality when accompanied by a local decrease in cerebral blood flow.[2]
The Blood and Blood Component Injection Models in Rats
When modeling SAH, the pressure of the blood exposure should resemble that of the brain during a clinical episode. It is theorized that when SAH occurs, arterial pressure can be anywhere from 20-40 times higher than the normal intracranial pressure. Therefore, animal models of hemorrhage that are induced via blood injection are divided into two categories, namely:
- Arbitrary pressure models
- Pressure-control models
These two types of models are two different options for how the pressure of the blood that will be injected into the experimental animals is controlled.
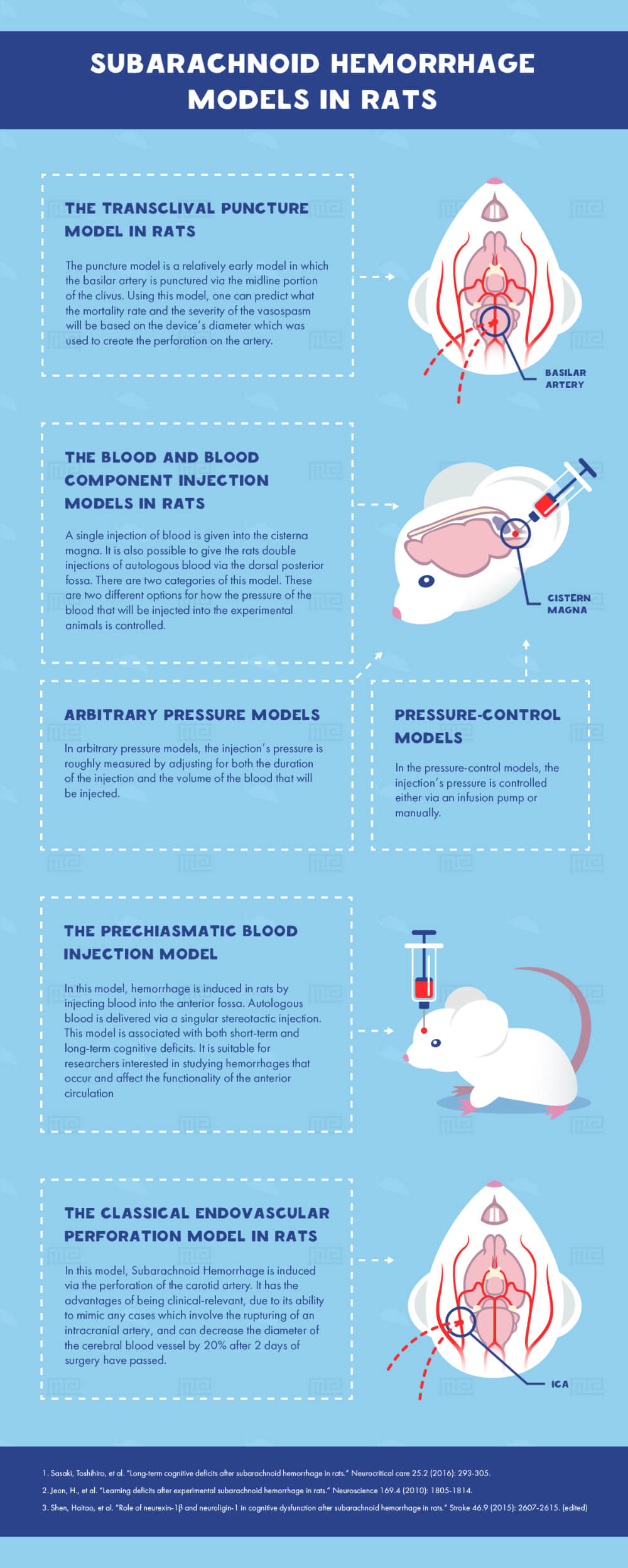
In arbitrary pressure models, the injection’s pressure is roughly measured by adjusting for both the duration of the injection and the volume of the blood that will be injected. In the pressure-control models, the injection’s pressure is controlled either via an infusion pump or manually.
Once a single injection of blood is given into the cisterna magna (often referred to as the ‘single-hemorrhage’ model), it is common to observe a biphasic vasospasm and the mortality rate for a single injection is about 11.5% with the rats’ vasospasms returning to control levels around 24 hours post-injection.
It is also possible to give the rats double injections of autologous blood via the dorsal posterior fossa. By giving the second injection 48 hours after the initial one, biphasic vasospasms will also occur, but it will not lead to neurological deficits. However, if the two injections are spaced 24 hours apart, then neurological deficits can be observed in the subsequent days. The double injection model is consistently associated with long-term cognitive deficits.[3][4][5]
Some of the disadvantages of the blood and blood component injection animal models of hemorrhage include the increased risk of damaging cerebral tissues due to the mechanical procedures needed to perform the injections and the lack of control in how the blood distributes through the blood vessels.
The Prechiasmatic Blood Injection Model
Alternatively, it is also possible to induce hemorrhage in mice by injecting blood into the anterior fossa.[6] Autologous blood is delivered via a singular stereotactic injection. This model is associated with both short-term and long-term cognitive deficits.[7][8] Injecting blood into the prechiasmatic cistern primarily affects the anterior circulation path of the brain, so this model is suitable for researchers interested in studying hemorrhages that occur and affect the functionality of the anterior circulation. However, the major downside of this model is the high mortality rate. It is hypothesized that the high mortality rates associated with this model are due to the small volume of the prechiasmatic cistern and the hemorrhagic location.
Prechiasmatic vs. Double Blood Injection Models
In a study that compared long-term cognitive deficits between double blood injection and prechiasmatic blood injection animal models of subarachnoid hemorrhage, behavioral and cognitive differences (as well as similarities) were noted.[6]
Prior to SAH induction via the two animal models of hemorrhage, there were no differences in the Rotarod test, which is a motor coordination test that was given two days before the experimental modeling had begun in order to measure motor abilities. After the models were induced, group differences were observed between the models and their respective controls only. The double blood injection model had a shorter latency time than its control (double saline injection) and the prechiasmatic blood injection model had a shorter latency time than its control (prechiasmatic saline injection) on the first day of testing after model-induction had occurred. By day 35, group differences returned to control values, indicating that Rotarod-measured behavioral changes occurring as a result of SAH induction are temporary and short-term in nature.[6]
Next, anxiety-levels were compared between the two SAH models of hemorrhage by means of measuring behavior with the Elevated-Plus Maze. Anxiety was of interest because in clinical cases, there is high variability reported by SAH patients. In these patients, anxiety disorders have been measured to have an estimate ranging upwards of a 40% incidence rate.[9][10][11][12] Therefore, anxiety is highly relevant to the neuropsychological profile of patients that have experienced a SAH.
In the prechiasmatic blood injection model, there were more open arm entries than in the double blood injection model. The double blood injection model, however, was associated with increased time spent in the maze’s closed arms, indicating higher anxiety levels. The researchers interpreted these behavioral discrepancies due to differences in brain region injuries. The prechiasmatic blood injection model (where the mice had more open arm entries and greater time spent in the open arms) predominantly causes injury to the medial prefrontal cortex. So, the researchers interpreted the resulting behavior as being translational and consistent with patients that have sustained an injury to this region, profiled by behaviors such as increased risk-taking and poor decision-making abilities. By contrast, the double injection model (in which the mice were in the closed arms for the majority of the time) causes injury to the hippocampal CA1 region, but the researchers found this combination of behavior and injury to be inconsistent with previous studies. Therefore, more research is necessary, in order to elucidate the complex connection between behavior, cognition, and regions of insult due to hemorrhaging.
Single vs. Double Injection Models for Inducing SAH in Rats
A different study compared the cognitive effects between the double-injection and single-injection methods for inducing subarachnoid hemorrhage in rats. Behavioral tests were given 3 weeks after the original SAH-induction. In the Open Field Test, only the rats that received a double-injection of blood showed statistically significant behavioral changes. They spent less time in the open, middle part of the field, had decreased average velocity, and decreased travel distance. In the Forced Swim Test, both the single- and double-injection rats showed significant changes in behavior as revealed by prolonged immobility time when compared to the control group. Both of the models, single- and double-injection, caused deficits in behavior in some regard. Of note, the double-injection method led to more severe deficits than the single-injection method, but both methods created significant behavioral impairments as compared with controls that received saline injections.[5]
The Classical Endovascular Perforation Model in Rats
SAH can be induced via the perforation of the carotid artery, a classical approach that was established in 1995 by Bederson et al.[13] and then modified by Veelken et al.[14] in the same year. This animal model requires surgical precision in order to perforate the internal carotid artery close to where it bifurcates. It is accomplished by using a sharp suture with a diameter that is about 200-250 μm through the external carotid artery. This model has the advantages of being clinical-relevant, due to its ability to mimic any cases which involve the rupturing of an intracranial artery, and can decrease the diameter of the cerebral blood vessel by 20% after 2 days of surgery have passed.
The weaknesses of the endovascular perforation model in rats are high mortality rate (about 37 to 50% at 24 hours post surgery), surgical failures to induce the model (at about 12%), and lack of control over subsequent blood distribution.[2]
The Modified Endovascular Perforation Model
One group of researchers compared the classical endovascular perforation technique with its more contemporary version (known as the modified endovascular perforation technique). The two techniques are quite similar. However, the modified version makes use of a filament (a tungsten wire, to be more specific) that is only 80 μm in diameter to perforate the internal carotid artery. This feat is accomplished by means of surgically inserting a polytetrafluoroethylene (PTFE) tube into the carotid artery and then guiding it upwards until it reaches the internal carotid artery. At this point, the inner filament would perforate the vessel. Then, the PTFE tube is removed and the carotid artery sealed, but the perforation in the internal carotid remains, in order to induce modified endovascular perforation animal model of hemorrhage. It is important to note that while the classical perforation model perforates with a filament that is 200-250 μm, the modified method uses one that is 80 μm in diameter, so a research study was conducted whether such differences in methodology would have an impact on the subsequent animal model, including the animals’ behavior and cognition.[15]
When comparing the two models, a few statistically significant differences were established by Hollig et al.[16] The two models created different peak intracranial pressure levels, with the classical model having 94 +/- 23 mmHg and the modified perforation model resulting in the peak pressure of 68 +/- 19 mmHg. Furthermore, there were fewer incidences of damage, mistakes, and subdural hematomas noted in the rats that underwent surgery for the modified perforation model, indicating that this model has less confounding variables than the classic method.
SAH Models In Mice
Alternatively, mice can also be used to model subarachnoid hemorrhage. In fact, several advancements have been made in modeling mouse models of hemorrhage, based on rat models of hemorrhage, including the perforation model.
However, mice are a little bit more challenging to use and manipulate for inducing hemorrhages, since they have a smaller cranial size than rats do, but there are still a few options available.
The Endovascular Perforation Model in Mice
Kamii et al. modified the perforation rat model so that it would be suitable for mice. They used a smaller filament size, in order to perforate the anterior cerebral artery. The result was diffused blood distribution throughout the brain’s basal cistern.[17] One research group, guided by this mouse animal model of hemorrhages, observed the mortality rate as being 20-29% in non-transgenic mice and about 19-27% in transgenic mice. A different group reported that there is an 11.1% (affecting every 4 in 36 mice) mortality rate in wild-type mice as a result of the surgical procedure needed to inflict this model. The most severe vasospasm reported using this method was found about 72 hours after induction with a 57% decrease in diameter as measured by the cerebrovascular casting method.[17] Severe neurological deficits have been established in this model at the 24 and 72 hour marks post SAH induction via perforation, as measured by the neurological score.[18][19]
This model, however, has received mixed criticisms due to its inability of creating neurocognitive deficits as observed in rats under the same model.[20] For example, one study demonstrated that the SAH induction in mice via surgical perforation failed to induce neurocognitive deficits in the Morris Water Maze. The mice with perforation surgery performed at the level of the control group and did not exhibit any deficiencies in learning or memory when it came to locating the hidden platform, as demonstrated by similar times to complete the maze.
Therefore, more research is necessary, in order to expand the knowledge available on how cognition is affected by this particular animal model of hemorrhage.
The Murine Cisterna Magna Blood Injection Model in Mice
This model, developed by Lin and collaborators,[21] is associated with minimal focal neurological deficits and low mortality rates. The blood injection occurs in the anterior cerebral artery and the basilar artery and also affects the middle cerebral artery. The model is still observable by day 2 and lasts until day 4 with absolute recovery from vasospasms occurring one week later. In this experiment, vasospasms were measured through the use of a computer-assisted image analysis system in which perfused brain samples were fixated with formalin and then infused with a mix of gelatin and India ink. Such analysis revealed that the arterial vasospasms in this model occur twice in the anterior cerebral artery, the basilar artery, and the middle cerebral artery. The first vasospasm occurs about 1-6 hours after induction and peaks at about 6-12 hours, then the second phase of observable vasoconstriction will persist for roughly 1.5-4 days.[2]
The murine cisterna magna blood injection model was developed based on the cisterna magna model in rats and thus also resembles its advantages and disadvantages. Some advantages are low mortality rate due to the lesser extent of brain damage. But, this model does not mimic the clinical manifestation of subarachnoid hemorrhage which is more devastating and uncontrollable in nature and includes the rupturing of blood vessels. However, this model is able to produce biphasic vasospasms clearly which are widespread and severe.
Hemolyzed Arterial Whole Blood Injection Model in Mice
It is also possible to induce hemorrhages in mice via the injection of hemolyzed arterial whole blood into the subarachnoid space, close to the neocortex, by creating a burr hole near the junction of the occipital and right parietal bones.[22] Such a model is handy for investigations that wish to focus on apoptotic mechanisms instigated after a SAH and can incorporate genetically manipulated mice.
Intracerebral Hemorrhage Animal Models
The other form of hemorrhage that is commonly studied is the intracerebral hemorrhage (ICH). An intracerebral hemorrhage refers to a bleed that occurs within the brain matter. The most common animal models of intracerebral hemorrhage are described below.
Injection of Bacterial Collagenase Induces ICH
By injecting bacterial collagenase into the blood vessels, researchers induce intracerebral hemorrhage using different principles than those in the injection of autologous blood. Collagenase’s enzymatic action causes a disruption in the blood vessels by acting on their basal lamina which in turn weakens the blood vessels and leads to blood leaks into the neighboring tissues.[23] While the blood injection method causes a single large bleed, which mimics some clinical situations but not all, injection of bacterial collagenase causes rebleeding or continued bleeding. Once a collagenase injection has been given, the bleeding lasts for hours and derives from a multitude of burst vessels. In contrast, the bleeding that occurs in the blood injection model is more concentrated in the area in which the injection was administered.[24]
So, the bacterial collagenase model for inducing a spontaneous hemorrhage is useful for researchers that wish to study hematoma enlargement and prolonged bleeding in the brain which occurs from the weakening of multiple, distributed blood vessels. It is also a useful model for researchers interested in developing treatments focused on re-establishing brain homeostasis. The major disadvantage of bacterial collagenase, however, is that it possibly amplifies the brain’s inflammatory response and produces overly high levels of neurotoxic effects.[24] Also, it is possible that these prolonged bleeds which occur as a result of bacterial collagenase administration may end up producing an ischemic cerebral injury which is an outcome that is not always consistent with human ICH.[25]
Injection of Autologous Blood Induces ICH
This model is similar to those used for inducing subarachnoid hemorrhage. However, instead of injecting into the cisterns of the brain, the injection of autologous blood is administered to a particular region of the brain and creates a single large bleed.[26] When injecting blood, a narrow lesion is created and blood is likely to move through vessels in which have the least amount of resistance, creating a stable and rapid hematoma.[24]
Developing More Animal Models for Intracerebral Hemorrhage
One of the major criticisms of the blood injection method revolves around the fact that most studies conducted to this date use a methodology in which the blood is injected into the striatum, a specific component of the basal ganglia. Realistically, intracerebral hemorrhages can occur anywhere in the brain, not just in the striatum. Therefore, in the recent years, special efforts have been made in order to develop reliable and reproducible models in which blood is injected in different brain regions.
For example, one group of researchers set out to create three models in which the blood injection method could be performed in the cortex, hippocampus, or ventricles of the brain. The study demonstrated that injecting blood in these regions led to reproducible effects in inflammation, brain edema, brain damage, and locomotor deficits. Cognitive and emotional deficits were observed in the mice that had a hemorrhage in the cortex or the hippocampus. Cognitive deficits were observed when the intracerebral hemorrhage occurred in the cortex, as revealed by increased times of immobility in both the Tail Suspension Test and the Forced Swim Test. Novel Object Recognition showed impairments in behavior in the mice with a hippocampal hemorrhage, since these mice spent equal times with a new and a previously introduced object.[27]
Hemorrhaging in Obese Versus Healthy Animals
Obesity is an increasingly pressing public health issue that is associated with a specific biological profile. Since adipose tissue in obesity has certain characteristics, like increased M1 macrophage accumulation and an increased secretion of pro-inflammatory cytokines secretion,[28] it is important to have an animal model that mimics these characteristics.
Given the increased prevalence of obesity, research is currently investigating whether a hemorrhagic episode in an obese patient will have a different outcome and need a different treatment protocol than a hemorrhagic episode in nonobese patients.
In fact, there is a limited amount of research available that specifically studies the outcomes of obese patients after undergoing a hemorrhaging episode. However, this intersection, between obesity and hemorrhaging, is one that should warrant future scientific attention, especially since it has been demonstrated that the mortality rate from a hemorrhage proportionally increases alongside with body mass index. Furthermore, a high incidence of multiple organ failure has also been correlated with increased body mass index.[29] The positive correlation between body mass index, increased incidence of multiple organ failure, and traumatic hemorrhage indicate that there is an interplay between these obesity and hemorrhaging conditions and that future research should investigate the mechanisms and eventually improve existing treatment protocols.[30]
By using animals that biologically represent obesity, research can become more precise by taking into account the context in which hemorrhaging occurs.
First, inducing obesity must occur, either through dietary or genetic manipulation (it has been shown that simply altering any one of 250 obesity-related genes can experimentally induce obesity).[31] Usually, the dietary induction of obesity is more preferred since it more closely reflects the condition of human obesity. Obesity is induced either through chemical injections (like streptozotocin), through the high-fat diet (which is high energy density) or the “cafeteria diet” which induces hyperphagia and therefore obesity.[32][31]
Then, after an animal model of obesity has been selected, it can be combined with an animal model of hemorrhaging (like fixed-pressure or fixed-volume). For example, Matheson et al. subjected obese and lean rats to anesthetization and a fixed-pressure hemorrhage of 40% the rats’ mean arterial pressure for 60 minutes and found that the obese rats had impaired hepatic flow, increased kidney and liver injury, and increased systemic inflammation when compared to the lean rats that had hemorrhage.[33][34] Such findings indicate that physiology affects subsequent outcomes after a hemorrhagic episode.
Interestingly, this animal model (combining hemorrhaging and obesity) may eventually be extended to include Alzheimer’s disease in its framework. A recent study made use of APP/PS1 mice, mice that are genetically primed to develop Alzheimer’s disease (AD), and divided them into two experimental groups, one receiving streptozotocin injections (the obese group) and the other not. The researchers found that the obese AD mice had worse symptomology and a greater number of spontaneous bleeds than the non-obese AD group, indicating that obesity affects vasculature.[35] This negative trend extended to their cognitive performance as seen by decreased performance in the Novel Object Recognition, demonstrated by their inability to learn and remember novel objects.
Such a study, which examined both vasculature and cognition, shows the importance of studying hemorrhage within a certain context. This direction, focusing on hemorrhage within the specific context of obesity in Alzheimer’s-induced mice, should be explored by future research interested in identifying the mechanisms of the pathology and extended upon by researchers that wish to combine several animal models together.
More Topics in the Field of Hemorrhage Animal Model Research
Other reoccurring themes in the field of animal models of hemorrhage include:
- Methods for resuscitation, how hemorrhage is controlled, with the most common resuscitation fluids used being: saline, blood, colloids, or lactated Ringer’s
- Whether anesthesia is included or absent since anesthetic administration can subsequently affect physiological responses such as the hemodynamic response
- The use of anticoagulants like heparin
Consider anesthesia, for example, as to why it is a variable of interest in animal models of hemorrhage. Anesthesia hampers the sympathetic activity in experimental animals, yet is commonly used in clinical practice. However, when obese rats are given anesthesia they have an adrenergic and an altered hemodynamic response to anesthesia which in turn may affect the subsequent treatment that would follow as a result of a hemorrhagic episode. Therefore, more research is needed to study, in detail, how hemorrhaging and treatment outcome across different patient profiles are affected by clinically-relevant variables such as anesthesia, anticoagulants, or resuscitation.
Furthermore, since clinical hemorrhages are typically trauma-related, many experimental hemorrhage methods will extend to include blunt insults to body parts such as the chest, abdomen, head, and/or extremities, to the induction procedure.
Conclusion
For experimental purposes, the researcher must be familiar with all of the possible animal models of hemorrhage and pick the one(s) most suitable for answering the research question at hand.
In conclusion, animal models of hemorrhage are simultaneously well-established and still developing and offer a strong base for research to be conducted, in order to progress existing knowledge and clinical methods.
References
- Ikram, M. Arfan, Renske G. Wieberdink, and Peter J. Koudstaal. “International epidemiology of intracerebral hemorrhage.” Current atherosclerosis reports 14.4 (2012): 300-306.
- Titova, Elena, et al. “Experimental models of subarachnoid hemorrhage for studies of cerebral vasospasm.” Neurological research 31.6 (2009): 568-581.
- Takata, Ken, et al. “Long-term cognitive dysfunction following experimental subarachnoid hemorrhage: new perspectives.” Experimental neurology 213.2 (2008): 336-344.
- Takata, Ken, et al. “Simvastatin treatment duration and cognitive preservation in experimental subarachnoid hemorrhage.” Journal of neurosurgical anesthesiology 21.4 (2009): 326-333.
- Boyko, Matthew, et al. “The neuro-behavioral profile in rats after subarachnoid hemorrhage.” Brain research 1491 (2013): 109-116.
- Sasaki, Toshihiro, et al. “Long-term cognitive deficits after subarachnoid hemorrhage in rats.” Neurocritical care 25.2 (2016): 293-305.
- Jeon, H., et al. “Learning deficits after experimental subarachnoid hemorrhage in rats.” Neuroscience 169.4 (2010): 1805-1814.
- Shen, Haitao, et al. “Role of neurexin-1β and neuroligin-1 in cognitive dysfunction after subarachnoid hemorrhage in rats.” Stroke 46.9 (2015): 2607-2615.
- Morris, Paul Graham, JT Lindsay Wilson, and Laurence Dunn. “Anxiety and depression after spontaneous subarachnoid hemorrhage.” Neurosurgery 54.1 (2004): 47-54.
- Visser-Meily, JM Anne, et al. “Long-term health-related quality of life after aneurysmal subarachnoid hemorrhage: relationship with psychological symptoms and personality characteristics.” Stroke 40.4 (2009): 1526-1529.
- Fontanella, M., et al. “Neuropsychological assessment after microsurgical clipping or endovascular treatment for anterior communicating artery aneurysm.” Acta neurochirurgica 145.10 (2003): 867-872.
- von Vogelsang, Ann-Christin, et al. “Patients experience high levels of anxiety 2 years following aneurysmal subarachnoid hemorrhage.” World neurosurgery 83.6 (2015): 1090-1097.
- Bederson, Joshua B., Isabelle M. Germano, and Lorraine Guarino. “Cortical blood flow and cerebral perfusion pressure in a new noncraniotomy model of subarachnoid hemorrhage in the rat.” Stroke 26.6 (1995): 1086-1092.
- Veelken, Julian A., Rodney JC Laing, and Jan Jakubowski. “The Sheffield model of subarachnoid hemorrhage in rats.” Stroke 26.7 (1995): 1279-1284.
- Höllig, Anke, et al. “Experimental subarachnoid hemorrhage in rats: comparison of two endovascular perforation techniques with respect to success rate, confounding pathologies and early hippocampal tissue lesion pattern.” PloS one 10.4 (2015): e0123398.
- Kamii, Hideyuki, et al. “Amelioration of vasospasm after subarachnoid hemorrhage in transgenic mice overexpressing CuZn–superoxide dismutase.” Stroke 30.4 (1999): 867-872.
- Parra, Augusto, et al. “Mouse model of subarachnoid hemorrhage associated cerebral vasospasm: methodological analysis.” Neurological research 24.5 (2002): 510-516.
- McGirt, Matthew J., et al. “Simvastatin increases endothelial nitric oxide synthase and ameliorates cerebral vasospasm resulting from subarachnoid hemorrhage.” Stroke 33.12 (2002): 2950-2956.
- Fanizzi, Claudia, et al. “Minimal long-term neurobehavioral impairments after endovascular perforation subarachnoid hemorrhage in mice.” Scientific reports 7.1 (2017): 7569.
- Lin, Chih-Lung, et al. “A murine model of subarachnoid hemorrhage-induced cerebral vasospasm.” Journal of neuroscience methods 123.1 (2003): 89-97.
- Titova, Elena, et al. “Experimental models of subarachnoid hemorrhage for studies of cerebral vasospasm.” Neurological research 31.6 (2009): 568-581.
- Matz, Paul G., Miki Fujimura, and Pak H. Chan. “Subarachnoid hemolysate produces DNA fragmentation in a pattern similar to apoptosis in mouse brain.” Brain research858.2 (2000): 312-319.
- Rosenberg, Gary A., et al. “Collagenase-induced intracerebral hemorrhage in rats.” Stroke 21.5 (1990): 801-807.
- MacLellan, Crystal L., et al. “Rodent models of intracerebral hemorrhage.” Stroke 41.10 suppl 1 (2010): S95-S98.
- Krafft, Paul R., et al. “Modeling intracerebral hemorrhage in mice: injection of autologous blood or bacterial collagenase.” Journal of visualized experiments: JoVE 67 (2012).
- Bullock, R., et al. “Intracranial haemorrhage induced at arterial pressure in the rat: Part 1: Description of technique, ICP changes and neuropathological findings.” Neurological research 6.4 (1984): 184-188.
- Zhu, Wei, et al. “Mouse models of intracerebral hemorrhage in ventricle, cortex, and hippocampus by injections of autologous blood or collagenase.” PLoS One 9.5 (2014): e97423.
- Tchernof, André, and Jean-Pierre Després. “Pathophysiology of human visceral obesity: an update.” Physiological reviews93.1 (2013): 359-404.
- Hwabejire, John O., et al. “Body mass index in blunt trauma patients with hemorrhagic shock: opposite ends of the body mass index spectrum portend poor outcome.” The American Journal of Surgery 209.4 (2015): 659-665.
- Nelson, Jana, et al. “Obese trauma patients are at increased risk of early hypovolemic shock: a retrospective cohort analysis of 1,084 severely injured patients.” Critical care 16.3 (2012): R77.
- Speakman, John, et al. “Animal models of obesity.” Obesity Reviews 8 (2007): 55-61.
- Hariri, Niloofar, and Louise Thibault. “High-fat diet-induced obesity in animal models.” Nutrition research reviews 23.2 (2010): 270-299.
- Matheson, Paul J., et al. “Direct peritoneal resuscitation improves obesity-induced hepatic dysfunction after trauma.” Journal of the American College of Surgeons 214.4 (2012): 517-528.
- Matheson, Paul J., et al. “Obesity-induced hepatic hypoperfusion primes for hepatic dysfunction after resuscitated hemorrhagic shock.” Surgery 146.4 (2009): 739-748.
- Ramos-Rodriguez, Juan José, et al. “Increased spontaneous central bleeding and cognition impairment in APP/PS1 mice with poorly controlled diabetes mellitus.” Molecular neurobiology 53.4 (2016): 2685-2697.